
Learning about Post-Traumatic Stress Disorder (PTSD)
According to research studies conducted in the US, 3.6% of the adult population has Post-Traumatic Stress Disorder (PTSD) at any one time, with a lifetime prevalence of 6.8%. The prevalence of PTSD is higher among females at 5.2%, compared to males at 1.8%. Adults with PTSD commonly report suffering from a functional disability, with 36.6% experiencing serious impairment, 33.1% experiencing moderate impairment, and 30.2% experiencing mild impairment.
Typical examples of traumatic events that can trigger PTSD include sexual assault (with rape being the most common), military combat, physical violence, childhood abuse, natural disasters, road traffic accidents, the sudden death of a loved one, witnessing someone getting seriously injured or killed, terrorist attacks and mass shootings.
In Singapore, up to 13% of road traffic accident (RTA) survivors experience acute stress disorder (ASD) within one-month post-RTA, and up to 21% develop symptoms of ASD. Up to 78% of trauma survivors without intervention may develop PTSD within one month after the RTA.
Symptoms
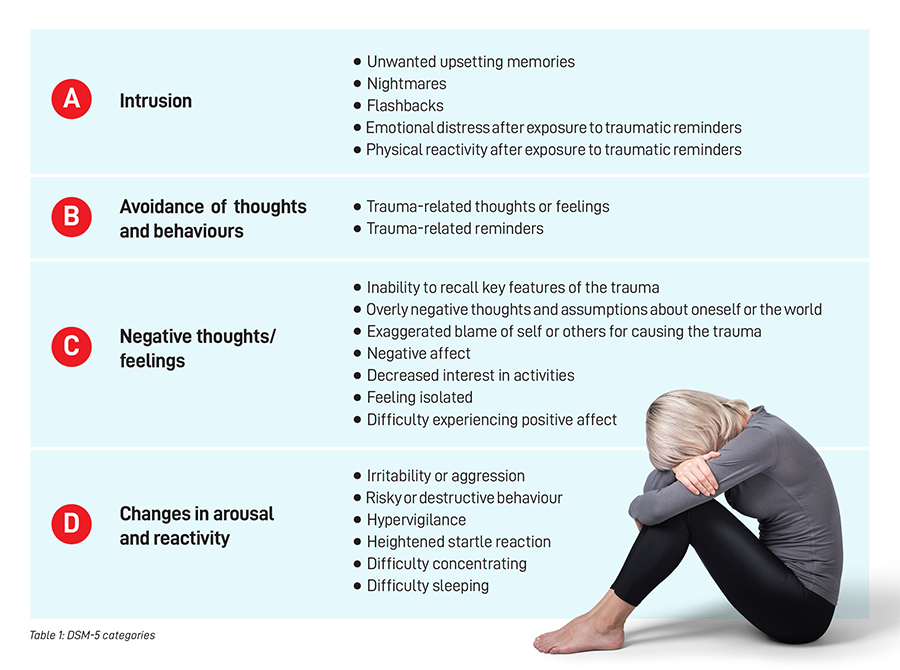
PTSD is a mental disorder that may develop due to direct or indirect exposure to violent or threatening events. The symptoms of PTSD can last for more than one month and are classified into four categories by the Diagnostic and Statistical Manual of Mental Disorders - Fifth Edition (DSM-5):
- Intrusion
- Avoidance of thoughts and behaviours
- Negative thoughts or feelings
- Changes in arousal and reactivity
Risk Factors
Several risk factors can contribute to the development of PTSD. These include having pre-existing mental health conditions (such as depression or anxiety), having a family history of mental health conditions, being in a job with high exposure to traumatic events (such as uniformed personnel e.g., combat soldiers), having limited adaptive coping strategies, and having little social support.
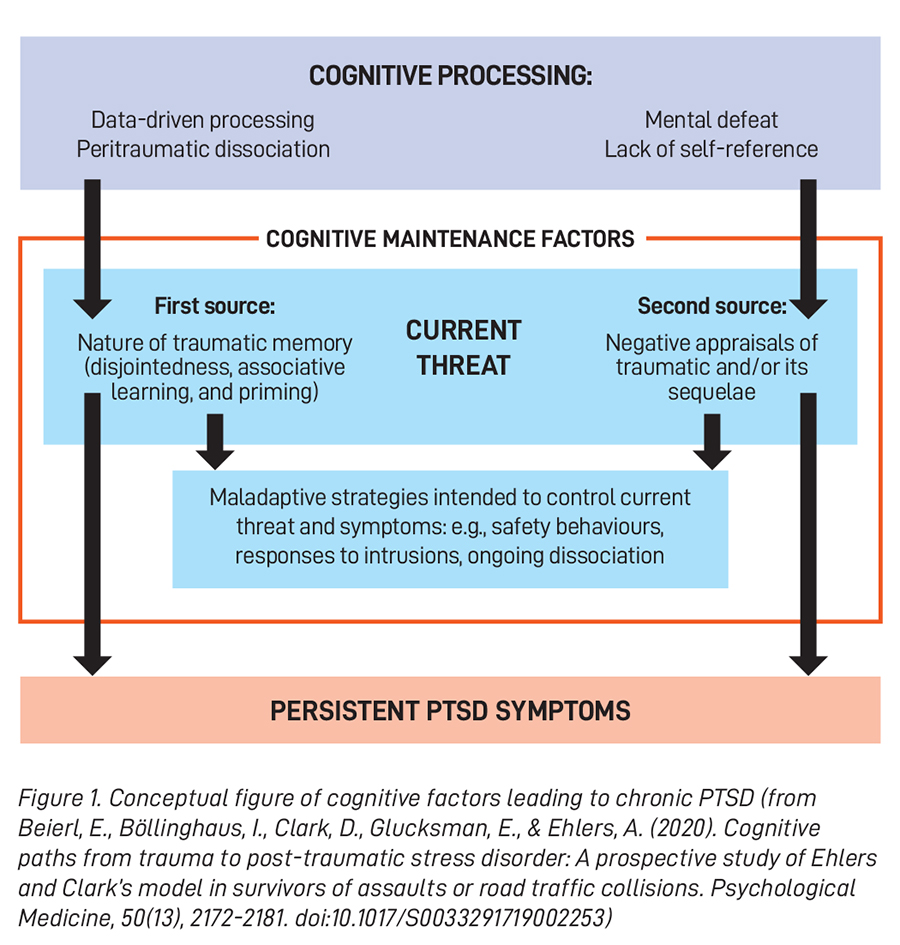
While some people recover from their PTSD symptoms within six months, the condition can become chronic for others. According to Ehlers and Clark’s model of PTSD (see Figure 1), chronic PTSD can develop if trauma survivors identify serious current threats through the traumatic event. The current threat is identified if trauma survivors process the trauma through the following sources:
- Disjointed trauma memory - Poorly linked information about the trauma may potentially misconstrue the trauma survivor’s trigger of the memories.
- Excessive negative appraisals of the trauma or its consequences - These negative appraisals commonly include those of self (“I am inadequate”) and others (“people cannot be trusted”).
It was assumed that memory characteristics and negative appraisals have a reciprocal relationship. Ehler and Clark’s model of PTSD further suggests that the sense of current threat consequentially encourages a series of maladaptive coping strategies to reduce the current threat but maintain the symptoms. These maladaptive strategies included excessive safety behaviours (such as excessive precaution), ineffective responses to intrusive memories (such as thought suppression and internal numbing), and persistent dissociation.
 PTSD and the Human Brain
PTSD and the Human Brain
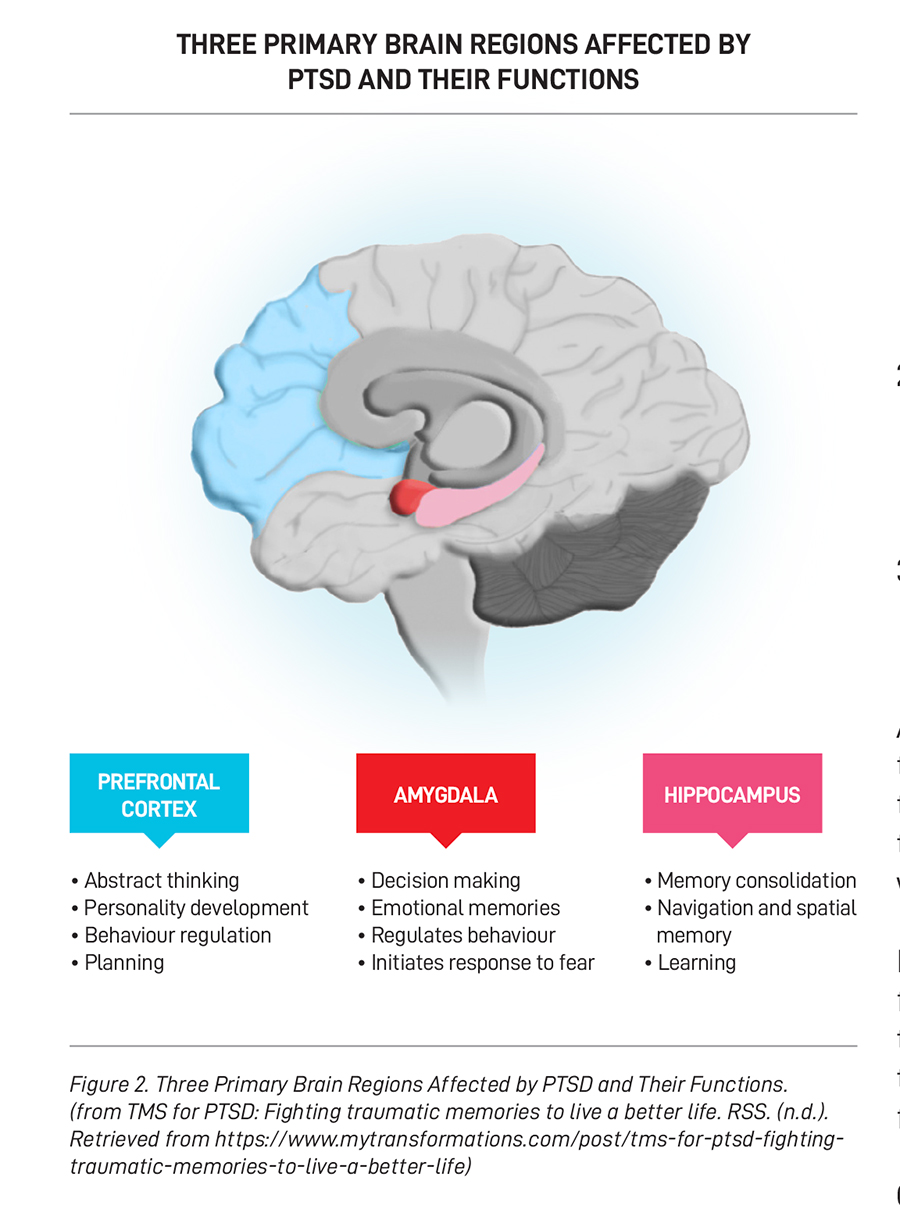
Many studies have investigated the implication of trauma to the brain to enhance the treatment plan for PTSD patients. According to scientists, PTSD patients often exhibit underactivation in the prefrontal cortex (the “executive functioning centre”). On the other hand, the amygdala, which is the “centre for emotion: fight-or-flight response”, becomes overactivated, which leads to inappropriate response patterns. Although the hippocampus of PTSD patients tends to be smaller than usual, it is found to be more active in response to perceived dangers. Following an increase in a reactive startle response, more norepinephrine is released in the body (which is typically released in the presence of perceived threats), and the patient’s brain functioning could be affected through the following ways: hyperarousal/hypervigilance, difficulty regulating emotions and impulsive behaviours, and slower processing response.
Treatments
PTSD is typically treated using medication, psychotherapy or a combination of both. Antidepressants are often prescribed to address trauma survivors’ sleep concerns, along with other medicines. There are various psychotherapy modalities used in the treatment of PTSD, some of which include:
1. Trauma-Focused Cognitive Behavioural Therapy (TF-CBT)
- Psychoeducation on reactions to trauma, strategies for managing arousal and flashbacks, and safety planning.
- Affective regulation and relaxation.
- Processing: Cognitive (trauma memories) and affective (trauma-related emotions, including shame, guilt, loss and anger).
- Cognitive restructuring of unhelpful thoughts.
- Helping patients manage their fears by exposing them to the feared situation (in the absence of danger).
- Enhancing future safety and development.
2. Exposure Therapy
Helping patients manage their fears by exposing them to the feared situation (in the absence of danger) and recounting the details of the trauma through media or visual imagery.
3. Eye Movement Desensitisation and Reprocessing (EMDR)
A standardised trauma-focused procedure using bilateral physical stimulation (eye movements, taps, or tones).
Although studies have found that early intervention of brieftrauma- focused cognitive behavioural intervention can help to reduce the severity of symptoms, it is also important to note that psychotherapy may not be helpful for trauma survivors who are in shock and distress.
In addition to individual psychotherapy for trauma survivors, family therapy that teaches family members how to support those suffering from PTSD can also help treat patients with their condition. This is because support from friends and family is one of the key factors in PTSD treatment.
Conclusion
In conclusion, PTSD is extremely common, and while the survivors may appear physically well, the psychological impact of trauma can be significant. However, early psychological intervention and adequate social support can effectively reduce the lasting impact of psychological trauma on trauma survivors.
Ms Adeline Tan is a registered Clinical Psychologist at Tan Tock Seng Hospital, who specialises in seeing adult patients with various mental health conditions such as depression, anxiety, obsessive-compulsive disorder and grief. She is also the lead psychologist of the Bariatric Clinic, providing psychological support for patients preparing for bariatric surgery.
